
Rhinoplasty
Rhinoplasty is one of the most sophisticated and technically demanding aesthetic surgical procedures. The results are worth the effort and may be stunning when precise planning is made that suits your facial proportions. It is neither possible to obtain someone else's exact nose shape with a rhinoplasty, nor will the nose you admired necessarily fit your face.
Every nose can be improved to the extent of its anatomic and proportional limits. The longevity of the results is closely related to the surgical techniques used, so choosing the best surgeon is the most important thing you can do for your nose-job. Dr. Demirkan has extensive experience in rhinoplasty with decades of patient follow-ups, and can combine several surgical approaches to give you the finesse and artistry you desire.

Is There a Nose Shape Ideal for Everyone
There is no standard description for an ideal nose shape that will fit everybody. Beauty standards and preferences for nose shape can vary significantly among individuals and cultures. In South America, some patients may undergo rhinoplasty to augment their nasal bridges, unlike most North American and European patients who wish to have smaller and more straight noses. In Asia, rhinoplasty primarily aims to eliminate the depressed nasal shape and make it larger.
However, there is one universal rule that is valid for all beautiful faces: the nose should be in proportion with the other parts of the face, such as the chin and forehead, moreover, it should have good proportions within itself, as in the proportion of nose projection to its length. And if you ask a question like "What kind of a proportion is required?", the answer is in Da Vinci's Golden Ratio.
Based upon the Golden Ratio, it might be speculated that Asian women want to augment their noses because it is too small in comparison to their facial width and squared shape, and vice versa for Caucasian women.
When it comes to aesthetic rhinoplasty, there may not be a uniform definition of a beautiful nose; however, there is one thing that everyone uniformly agrees upon, and that is an "operated look" is not acceptable. There are some commonly appreciated characteristics that are often associated with an aesthetically pleasing nose shape for women and they all contribute to an un-operated look:

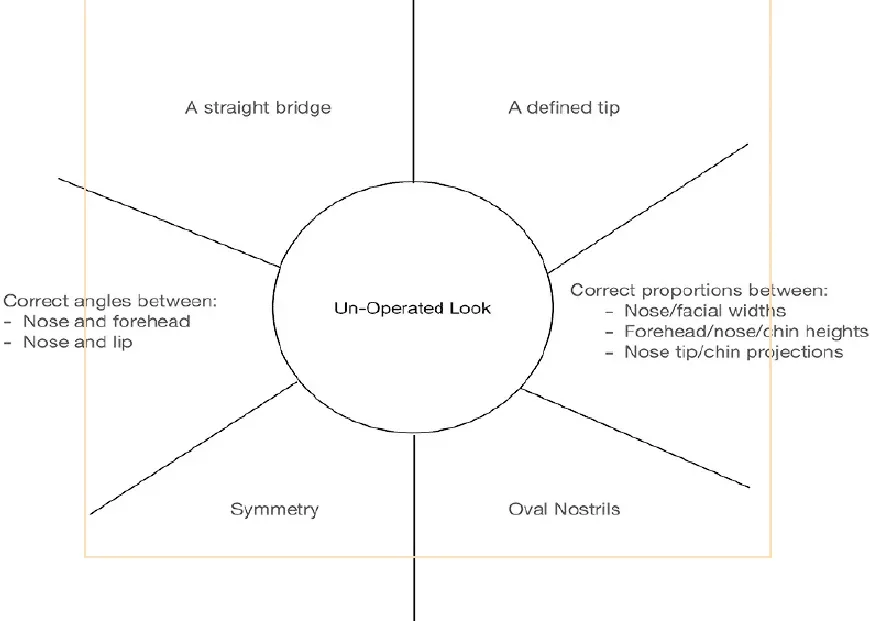
Operated look:
During your rhinoplasty consultation, Dr. Demirkan will consider your specific facial structure, discuss your desired outcome, and work with you to create a personalized surgical plan that aims to achieve your aesthetic goals while maintaining a natural appearance.

The Power of Rhinoplasty
Rhinoplasty has become a very powerful and detailed procedure when compared to what it was 15 years ago. There is a wide array of surgical techniques available now, which can alter many unfavorable features of a nose with natural and durable results. The following is a list of some problems for which patients commonly seek rhinoplasty:

Nasal deformities that can be corrected with rhinoplasty:
- Bulbous Tip
- Asymmetric Tip
- Upturned Nose
- Droopy Nose
- Crooked Nose
- Deviated Septum
- Broken Nose
- Low Bridge
- High Bridge
- Dorsal Hump
- Narrow Nose
- Wide Nose
- Wide or Flaring Nostrils
- Hanging Columella
- Nostril Collapse (nasal valve problems)
During your initial consultation, Dr. Demirkan will first ask you what do you not like about your nose, then he will add his suggestions regarding your specific facial proportions. Next, he will work with you on your simulation, to understand what you desire, and if it fits your face and physical properties. There may be features that cannot be changed, but yet affects the outcome, such as the thickness of your skin.
As a surgeon with tremendous experience in rhinoplasty, Dr. Demirkan will understand all of your concerns, will tell you about any drawbacks present, and will establish a realistic surgical plan that aims to achieve your aesthetic goals while maintaining a natural appearance.
Variables Affecting the Outcome in Rhinoplasty
Six factors outside surgical control shape your rhinoplasty result: skin type, age, scarring tendency, a crooked nose from childhood, facial asymmetry and ethnicity. Knowing them upfront helps set realistic goals and understand what the possible outcome will be, because some features cannot be altered with current surgical techniques.
Skin Type
Age
Scarring Tendencies
A Crooked Nose from Childhood
Facial Asymmetries
Ethnicity
What Are the Types of Rhinoplasty?
Rhinoplasty is classified in five ways: by incision (open or closed), by surgical philosophy (structural or preservation), by area of focus (tip, septum or both), by the number of previous surgeries (primary, revision or tertiary), and by surgical versus non-surgical approach. It is also the oldest type of aesthetic surgery, with a centuries-old history of continuous evolution in technique.
You may find many types of rhinoplasty procedures while searching the internet, and this might create confusion about their meaning and value, sometimes leading to comparisons of apples and oranges. Here is a quick guideline for the rhinoplasty types and the jargon:
Based on the incision site:
| Open Rhinoplasty | Closed Rhinoplasty | |
|---|---|---|
| Incision | Small incision across the columella plus internal incisions | Entirely inside the nasal passages, no external incision |
| Surgical access | Detailed view of the nasal anatomy; wider range of techniques | Limited exposure; columellar vessels preserved |
| Best suited for | A variety of concerns and more complex cases | Selected, less complex cases |
| Recovery | Standard | Potentially faster, particularly in the tip region |
Based on the surgical philosophy:
| Structural Rhinoplasty | Preservation Rhinoplasty | |
|---|---|---|
| Approach | Rebuilds a stable, balanced framework | Preserves the existing nasal structures as much as possible |
| Dorsal hump | Excised and a new dorsum recreated | Lowered (not excised) by removing part of the underlying septum |
| Grafts | Often cartilage grafts from the septum, ear or rib | Minimal grafting |
| Goal | Correct deviation and strengthen deficient cartilage | Retain the natural dorsal shape |
Based on the area of focus:
Tip Rhinoplasty
It is a specific type of rhinoplasty procedure that focuses on altering and enhancing the appearance of the nasal tip. It aims to achieve a more refined, balanced, and aesthetically pleasing tip shape without any interference with the nasal bones, dorsum, hump, or septum.
Septoplasty
It is a surgical procedure that aims to correct a deviated septum, which can cause various nasal issues, including breathing difficulties, congestion, recurrent sinus infections, and nasal blockage. The deviated portion of the septum is then straightened, reshaped, or removed to create better alignment and improve nasal airflow. It does not involve any shape-changing procedure in the external nose, maybe except in the columella region.
Septorhinoplasty
In cases in which the septal deviation is reflected externally as a deviation in the axis of the nose, then a rhinoplasty has to be added to correct the deviated nasal bones and asymmetric nasal soft tissues.
Based on the number of previous surgeries:
Primary Rhinoplasty
It refers to the first-time nasal reshaping surgery performed on a patient who has not undergone any previous nose surgeries.Secondary (Revision) Rhinoplasty
Also known as revision rhinoplasty, it is a corrective procedure performed after a previous rhinoplasty surgery. It is conducted to address unsatisfactory outcomes, complications, functional issues, or aesthetic concerns that may have persisted or developed following the initial surgery. Revision rhinoplasty can be more complex than primary rhinoplasty because it involves working with altered nasal anatomy and scar tissue from the previous surgery and frequently requires cartilage grafting from different sources.Tertiary Rhinoplasty
This refers to a subsequent corrective surgery performed after a previous revision rhinoplasty. It is typically conducted in cases where further modifications or corrections are required due to persistent or recurring issues following previous surgeries. It is much more complex and may have limited success.
Non-Surgical Rhinoplasty:
Non-surgical rhinoplasty, also known as liquid rhinoplasty, is a procedure in which the shape of the nose is altered without the need for surgery. Instead of making incisions, injectable fillers are used to modify the nasal contours and achieve the desired aesthetic outcome. It is a quick and minimally invasive procedure that typically takes less than 30 minutes to perform. However, it is useful only in a small group of selected patients with suitable nasal anatomy to:
- Correct small bumps or irregularities on the bridge of the nose.
- Enhance the projection of the nasal tip.
- Give a lifted appearance to a drooping nasal tip.
- Reduce a prominent nasal bridge.
A filler injection always adds volume, so a successful result is an illusion rather than a real reduction. It does not correct functional problems, the hyaluronic acid eventually disappears, and the nose is one of the facial danger zones where inadvertent intra-arterial injection can cause serious complications.

Male Rhinoplasty
Male rhinoplasty can differ from female rhinoplasty in terms of facial evaluation and planning, to protect the masculine look.

For men, a more masculine appearance is typically sought, which may be obtained by:
- Maintaining a straighter nasal bridge without a prominent supra "tip break-point"
- A higher-located nasofrontal angle (the deepest part of the transition between the forehead and nose) between the brows
- A stronger nasal profile by preserving a slightly wider nasal bridge and ensuring adequate nasal width
- Less projected or refined nasal tip
- Chin and/or mandibular angle augmentation with implants if necessary
Female rhinoplasty, on the other hand, often aims for a softer, more feminine nose, with a slightly curved or sloped nasal bridge and a more delicate, defined nasal tip.
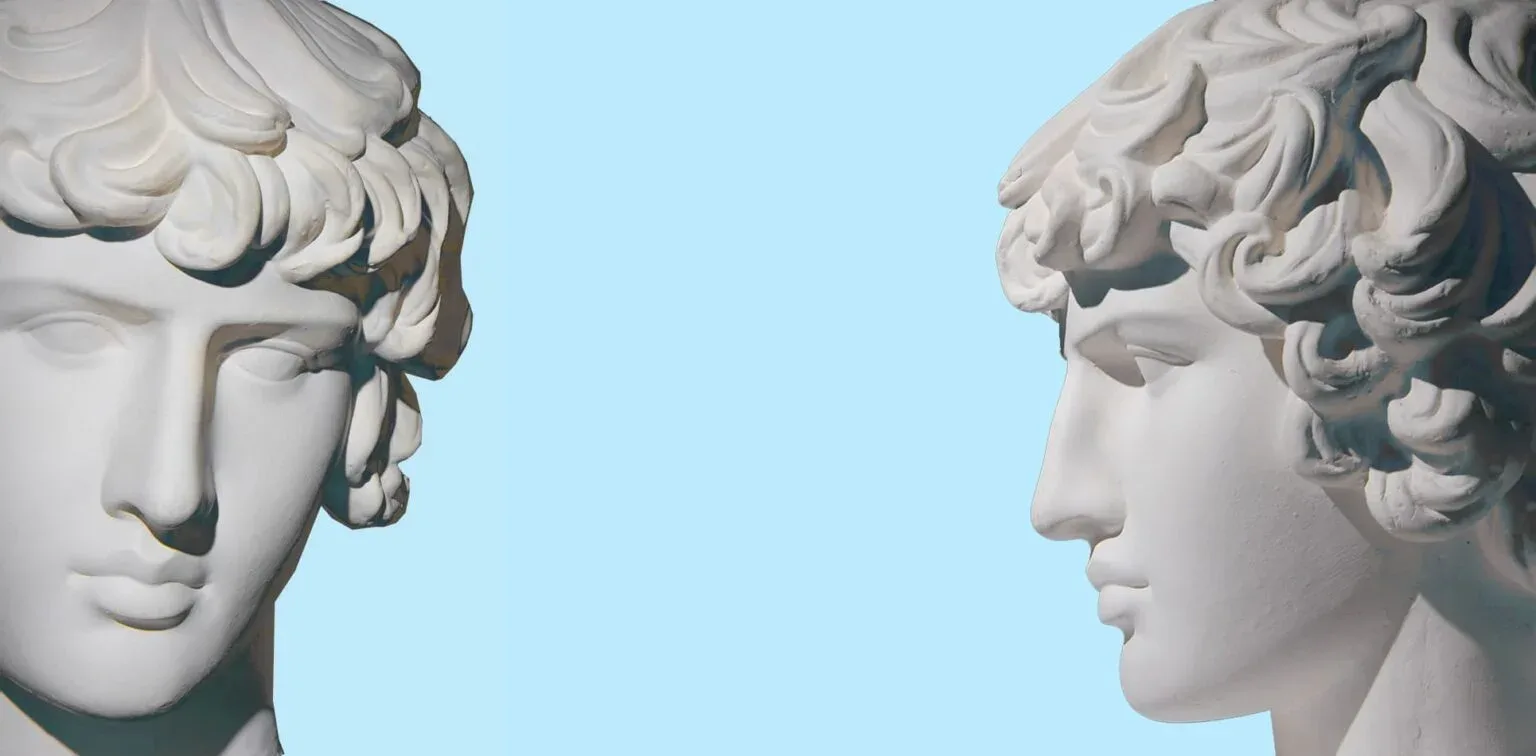
There is no standard nasal shape when it comes to men
There is no standard nasal shape for men, and the operation may be planned just to elevate a drooping tip while maintaining the nasal hump, or just to make the nose a bit smaller without changing the shape at all.
If a smaller nose is desired, it should be balanced with the other stronger anatomical features and facial proportions of the male gender, such as prominent cheek and jaw bones, low-set eyebrows and a prominent chin (like the man on the left side in the upper photo). In a face that does not have these strong features (like the man on the right side), a smaller, finely defined nose may cause feminization. While there are some key differences in the desired outcomes, the overall principles and surgical techniques of rhinoplasty apply to both men and women.

Simulation in Rhinoplasty
Simulation plays a valuable role in rhinoplasty by providing a preoperative visualization of potential surgical outcomes and aiding in surgical planning. Dr. Demirkan would like to communicate with you visually over your computer-generated simulation, to help you better understand what can be achieved through rhinoplasty. This will also enable you to express what you really want and understand what should you expect.
The simulation also allows Dr. Demirkan to evaluate the proposed changes in the context of your overall facial harmony. By visualizing the virtual nose alongside other facial features, he can assess the balance and proportionality of the anticipated result with your cheekbone, upper lip, and chin, and discuss the necessity of additional corrections in these areas if necessary.
Simulation is valuable in assisting the surgeon in planning the surgical approach and techniques required to achieve the desired results, as well.

Rhinoplasty and Breathing Problems
Rhinoplasty is an aesthetic procedure aiming to improve the nasal shape. However, the nose has an important role in breathing, and conditions deteriorating the breathing function such as septum deviation, allergic polyps, or sinusitis are not rare in people searching for an aesthetic improvement.
Dr. Demirkan will take a detailed history of your breathing problems during your initial consultation. He may order additional tests or ask for a consultation from his ear-nose-throat surgeon partner, if necessary.
After finding out the exact cause(s) of your nasal breathing problems, Dr. Demirkan will create an individual treatment plan for you that includes solutions for both your aesthetic and functional issues. According to the reason(s) of your nasal obstruction, this plan may include a one-session surgical treatment, a surgical treatment that is preceded by a medical treatment or a surgical procedure followed by a medical treatment.

Some examples of the treatment plans in cases with breathing problems are as follows:
- If you have only a septum deviation, Dr. Demirkan will perform a septoplasty during your aesthetic rhinoplasty.
- If you have an internal or external valve insufficiency, Dr. Demirkan will treat it with cartilage grafts during your rhinoplasty.
- If you have a concha bullosa, which means that one or more of your nasal turbinates have a bony cystic malformation from your birth, an ENT surgeon will perform a turbinate reduction in the same session with Dr. Demirkan, during your rhinoplasty.
- If you have a sinusitis problem, an ENT surgeon will join your rhinoplasty and perform an endoscopic sinus surgery. If you have allergic rhinitis with polyps, which means that it is really advanced, then you will need medical treatment for about 6 weeks prior to your rhinoplasty. You need to continue the anti-allergic treatment after the surgery as well unless you identify and remove the allergen(s) totally from your life.
- If you have mild allergic rhinitis you may have your rhinoplasty and continue with the anti-allergic medication after the surgery.

Rhinoplasty with Chin Augmentation or Reduction
Chin augmentation or reduction can be performed in conjunction with rhinoplasty to achieve facial balance and harmony. There is a close relationship between our perception of facial beauty and the chin-nose proportion. A nose that is too prominent or too recessed can change how the chin appears. For instance, a large or protruding nose may make a moderately projecting chin appear smaller, while a small nose might make a weak chin seem even weaker.
In a similar fashion, a weak or receding chin can make the nose appear more prominent and throw off the overall facial harmony. Therefore Dr. Demirkan will always check your facial proportions and offer you a concomitant chin surgery, when necessary. It may be best to analyze the possible outcome in a facial simulation.
A simple aesthetic rule to understand whether your chin is in balance with your nose is to look at the relative position of the nasal tip to your lips and chin. If you draw an oblique line in front of your face such as this, the tip of your nose should touch this line first, next should be your upper lip, then your lower lip, and finally the tip of your chin. If your chin is way back in this alignment you may need an augmentation with an implant. If the chin is touching this line together with the tip of your nose, then most likely it has to be taken back.
Chin Augmentation
The treatment for a weak chin is an augmentation genioplasty. Most of it is performed by insertion of a bone-like synthetic implant to the tip of the chin through a small incision under the lower teeth. There are different sizes and shapes of these implants for men and women. Another way of correcting a recessed chin is to inject hyaluronic acid fillers. However, the correction done by this method has a limited effect as the protrusive force exerted by fillers cannot be as strong as a solid implant. If overdone, the chin may look funny due to the flexibility of the filler augmented part.
Chin Reduction
A prominent chin deformity may be treated by a setback genioplasty, in which the tip of the bony chin is cut horizontally and set backward, and fixed with a plate. Smaller problems may be solved by bone shaving by piezo devices.
When there is a weak or protruding chin, which is going to be treated by surgery, it is important to rule out any associated dental occlusion problems. If the closure of the upper and lower teeth is disturbed as well, then the treatment plan may change completely.

Piezo and Microsaw Use in Rhinoplasty
Piezo devices have revolutionized the field of rhinoplasty by offering precise and controlled bone sculpting during the procedure. These devices utilize ultrasonic vibrations to cut through bone while minimizing trauma to surrounding tissues. This creates a huge difference when compared to the chisel-hammer bone fracturing of old times.
The impact of piezo devices can be significant
- Enhanced precision in bone cutting and shaping, leading to better results with fewer complications.
- Minimal trauma to the surrounding tissues during osteotomy (bone cutting), as this energy is selectively targeted to the bone.
- Less edema and bruising after the surgery due to decreased fracture trauma.
- Increased the ability of surgeons to perform extra moves that were not possible before the piezo era, such as multiple bone cuts, bone narrowing, and polishing.
The impact of piezo devices ultimately depends on the surgeon's skill and expertise, as well as their ability to combine this technology with other surgical techniques to achieve optimal results. Dr. Demirkan uses this technology successfully in all of his cases since 2016.
Microsaw devices, also known as oscillating saws, reciprocating saws, or micro-motor devices are another technological advancement used in rhinoplasty procedures. These instruments employ high-frequency oscillations to perform precise bone cutting. Their benefits are similar to those of piezo devices. However, their precision is a bit less than the piezo devices and are not selective for bone, and may cause more collateral tissue trauma.
Microsaw devices were available earlier than the piezo devices in rhinoplasty. Dr. Demirkan used them intensively between 2010 and 2016 but now prefers piezo.

How to Prepare for a Rhinoplasty?
Preparing for a rhinoplasty involves several important steps to ensure a smooth and successful procedure. Here are some general guidelines:

- Consultation with your plastic surgeon: You may arrange a live online consultation with Dr. Demirkan from this website. But before that, we advise you to send in your full medical history, your goals and concerns about the surgery, breathing problems if there are any, and facial photos (see guidelines for rhinoplasty photos). Dr. Demirkan will prepare a simulation before your consultation to provide you with a visual clue for the expected result while answering all your questions.
- According to the results of this initial consultation, Dr. Demirkan may ask for some tests or radiologic examinations, and may suggest an ear-nose-throat surgeon consultation depending on the extent of your breathing problems.
- When you decide about the surgery date, then you should quit smoking at least 15 days prior to this date, as smoking can increase the risk of complications and impair the healing process.
- Stop certain medications and supplements that may interfere with the blood clotting mechanisms: oral contraceptives and blood thinners such as aspirin and its derivatives, coumadin and heparin should be stopped 1-2 weeks before surgery; supplements such as Vitamin E, DHA and ginseng should also be stopped before the operation date.
- You may need to use certain anti-allergic sprays or medications before the surgery if indicated by your surgeon.
- If you are using glasses, they are not allowed for the first 6 weeks after a rhinoplasty due to the weight they exert on the fractured nasal bones. Therefore, it would be better to replace them with contact lenses, temporarily.
- It is suggested that you should arrive in Istanbul, 1 or 2 days prior to your surgery, to acclimatize.
- When you arrive in Istanbul, some blood tests will be performed at the hospital and an anesthesiology consultation will be performed. And Dr. Demirkan will see you once more in his office, where you will finalize your treatment plans. An ENT consultation may also be arranged if the ENT surgeon will also participate in your operation for breathing problems.
- Plan to stay at least 6 more nights in Istanbul after the surgery; you will stay at the hospital for 1 night after the operation.
- You may not need a companion for this surgery, however, the presence of a friend or a family member will be quite supportive when you are undergoing surgery, in a foreign country.

Postoperative Period
Most swelling settles over the first 2-3 months, and the nose reaches its final shape by around one year. The postoperative period is a crucial time for healing: compliance with medication, nasal cleaning, keeping the cast safe, tuning activity to your recovery pace, sun protection, the prescribed massages and protecting your nose from trauma all have significant effects on the final result.
The reaction to the operation is quite variable in each and every patient, depending on individual body responses. However, it should be noted that with the introduction of piezo devices, the collateral tissue damage is much lower during osteotomies (nasal bone fracturing), which is reflected in less edema and bruises in the postoperative period. The use of drainage in the osteotomy sites, silicone nasal stents with airways, and effective cooling devices following surgery have also contributed to decreased edema and bruising.

Immediate and Early Recovery Period:
- Right after the surgery, you will be taken to a recovery area where you will be monitored until the anesthesia wears off. You may experience some grogginess and discomfort during this time. It may be difficult to breathe from your nose due to internal packing or splints in your nostrils. They may create a pressure sensation as well.
- Your nose will be bandaged or have a cast. The internal splints will usually be removed on the 3rd postoperative day. The nasal cast will be replaced with a new one or removed on the 7th postoperative day.
- It is common to experience swelling, bruising, and nasal congestion in the first few days following the surgery. The best precaution to control swelling is the frequent application of cold packs to the nose and eyes. Arnica and bromelain tablets may also be useful for decreasing edema. To help reduce swelling, it is recommended to keep your head elevated while resting or sleeping and avoid activities that can increase blood flow to the face, such as strenuous exercise and straining.
- Pain and discomfort levels can vary among individuals, but it is common to experience some degree of discomfort usually due to the pressure of the internal nasal packing, and decreased ability for nasal breathing, especially in the first few days. Dr. Demirkan prescribes effective pain medication to relieve the pain related to surgery, and a prophylactic antibiotic.
- It is important to strictly follow the prescribed medication regimen, taking the medications as directed by your surgeon.
- Following the removal of your nasal packing, Dr. Demirkan will show you how to clean your nose and may prescribe nasal saline sprays to keep the nasal passages moisturized and promote healing.

Late Recovery Period:
- In this later recovery phase, you will experience a gradual reduction in nasal edema, however, it usually takes at least 2 or 3 months to reach the optimal phase. During that period Dr. Demirkan may ask you to do a nasal massage, if necessary. Please note that, if you have a thicker skin, your swellings will take more time to resolve.
- As there are controlled bone fractures during a standard rhinoplasty, your nose will not be structurally stable until after 6 weeks after the surgery. So, you have to protect it from any kind of trauma, should not use glasses, and should not sleep on your side or prone, during these 6 weeks period.
- Your nose may be numb for about 6 months after the surgery. It is normal, however, numbness may increase your chances of accidental nasal trauma.
- During the first 6 weeks after the surgery, activities that involve bending over, lifting heavy objects, or strenuous exercise should be avoided, as they can increase swelling and affect healing.
- You should be using effective sunscreens from the post-operative day 1 to the end of the 6 weeks recovery period, to prevent any post-inflammatory hyperpigmentation. This happens particularly in darker skin and in individuals who are exposed to the sun right after the surgery, and it usually settles under the eyes.
- The final shape of your nose will become visible at about the third month, following the resolution of the edema, however, changes in the nose shape continue till the end of the first postoperative year, at a much slower pace. Therefore, Dr. Demirkan advises you to wait until the end of the first year to see the final result.

Possible Complications in Rhinoplasty
Rhinoplasty is generally considered a safe procedure with a low risk of complications. However, as with any surgical procedure, there are potential risks and complications that can occur. It's important to note that the occurrence percentages can vary depending on various factors, including the complexity of the surgery, the surgeon's expertise, the number of revisions, and individual patient characteristics which are explained in the section of Variables in Rhinoplasty.
The informed consent form about the rhinoplasty procedure is available at the Rhinoplasty Surgery Informed Consent link. It is a list of all possible complications, however, it does not mean that each one of them will occur in your case with an equal probability. We will send you this consent form when you are looking for the surgery and ask you to read it and return it to us if you do not understand any part.
When you arrive in Istanbul, Dr. Demirkan will tell you which one(s) of this complication may be more likely in your case, following your physical examination. If your nasal anatomy and function are quite suitable for rhinoplasty, none of them may be likely to happen, as well. He will also explain to you the variables affecting your surgery, in order to set your expectation at a realistic level.
However, if you have an external nasal deviation that is coming from your childhood, have thick nasal skin, or if this is not your first rhinoplasty, you have more postoperative complication risk.

Frequently Asked Questions
Is rhinoplasty a painful procedure?
Do I need nasal packing in my rhinoplasty?
How long will the external splint stay after rhinoplasty?
How do I know if I need septoplasty?
What can I do to decrease swelling and bruising after rhinoplasty?
When can I get the result after rhinoplasty?
Is the result I get in my rhinoplasty stable?
Why is revision rhinoplasty more difficult to perform than primary rhinoplasty?
Is there an age limit for rhinoplasty? What is the best age?
Is open or closed rhinoplasty better for me?
Will my breathing problems diminish after the rhinoplasty?
Do I need grafts in my rhinoplasty?
What is the difference between ear and rib cartilage for a secondary rhinoplasty?
Related reading
Considering rhinoplasty?
Book a virtual consultation with Prof. Dr. Ferit Demirkan to discuss your goals and a plan suited to you.
Contact us